Pierre Mugabo1 ![]() ,
Richard Madsen2
,
Richard Madsen2
For correspondence:- Pierre Mugabo Email: pmugabo@uwc.ac.za Tel:+27219592190
Received: 13 September 2016 Accepted: 19 December 2016 Published: 01 February 2017
Citation: Mugabo P, Madsen R. Detection of drug-induced dyslipidaemia in HIV-positive patients treated with protease inhibitors in a South African district - A retrospective study. Trop J Pharm Res 2017; 16(1):239-244 doi: 10.4314/tjpr.v16i1.32
© 2017 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To determine whether protease inhibitors (PIs) cause hypercholesterolaemia and hypertriglyceridaemia, and to assess the influence of sex and age on serum total cholesterol (TC) and triglycerides (TG), and the level of adherence to therapeutic laboratory monitoring guidelines in HIV positive patients in the Eastern Health District, South Africa.
Methods: This was a retrospective study which compared baseline and follow-up TC and triglycerides serum levels in HIV-infected patients who received treatment, including PIs, between 2008 and 2012 in the Eastern Health District of the Cape Metropole Region (Cape Town, South Africa). Clinical and laboratory data were retrieved from patients’ folders and from a computerized database at National Health Laboratory Services (NHLS). The level of compliance with therapeutic laboratory monitoring protocols by health workers and patients was also assessed.
Results: Out of 753 patients (491 females, 262 males), 176 were 0 - 17, 465 were 18 - 44 and 12 were > 44 years old. The proportion of patients who had test results at the various time points ranged from 16.33 to 25.90 %, 17.66 to 24.83 %, 25.10 to 47.41 % and 25.23 to 36.79 % for TC, triglycerides, CD4 count, and viral load (VL) tests, respectively. There was a significant time increase (p = 0.0137) for serum TC from baseline to 3 years. For serum triglycerides, the overall time effect was not significant (p = 0.4132). There was a significant increase from baseline in CD4 and a significant decrease in VL during the study period. Sex and age did not show any relationship with TC and triglyceride serum levels.
Conclusion: This study demonstrated hypercholestrolaemia in HIV-infected patients receiving PIs. Age and sex did not have any effect on TC and triglycerides. Compliance with therapeutic laboratory monitoring guidelines was poor.
Introduction
Antiretroviral therapy (ART) has improved the prognosis of HIV-infection during the last decade. However, antiretroviral drugs are frequently associated with serious side effects including haematological, gastrointestinal, neurological, mental, skin and metabolic disorders [1].
Studies conducted in developed and developing countries have shown conclusive results that protease inhibitors (PIs) cause hyperlipidaemia [1-4]. About 60 % of HIV-positive patients develop hyperlipidaemia due to an abnormal lipid metabolism [5]. Hyperlipidaemia developing in HIV-positive patients may be due to the effect of PIs or HIV infection or the combination of both on the metabolism of lipids [6]. Stavudine and non-nucleotide reverse transcriptase inhibitors (NNRTIs) can also cause abnormal changes in lipid profile, but to a lesser extent than PIs [1].
According to the South African Department of Health (DOH) treatment guidelines, serum TC and serum TG are monitored at baseline, again at three months and then every year after starting PIs treatment. The protocol does not recommend follow-up of low density lipoprotein (LDL), very low density lipoprotein (VLDL) and high density lipoprotein (HDL) - cholesterol levels [7].
During the study period, the second line HIV-infection treatment for children included zidovudine, didanosine and Lopinavir /ritonavir. Children failing on this regimen were placed on abacavir, lamivudine and lopinavir/ritonavir. The second line treatment regimen for adolescents and adults included zidovudine, lamivudine and lopinavir/ritonavir [8].
Lopinavir/ritonavir were given at a fixed dose of 400/200 mg 12 hourly in adults and 230/57.5 mg/m2 12 hourly in children [9].
The objectives of this study were: To find out whether or not PIs cause hypercholesterolaemia and hypertriglyceridaemia in HIV-positive patients; to determine the influence of sex and age on TC and TG serum levels; and to assess the level of compliance with therapeutic laboratory monitoring protocols recommended by the DOH.
Methods
The project was designed as a retrospective study, comparing TC and TG serum levels at baseline, three months and every year for three years after initiating PIs. The study also assessed the level of compliance with therapeutic laboratory monitoring protocols by health workers and patients.
The study was conducted at five HIV clinics and one hospital, conveniently selected, in the Eastern Health District of the Cape Metropole region, South Africa. It involved exclusively HIV-positive patients of all ages and both sexes who were on treatment that included PIs for three years between 2008 and 2012. Patients were excluded from the study if any of the following applied: pregnancy, concurrent treatment with other drugs that can cause dyslipidaemia and concomitant diseases (e.g., diabetes mellitus) which interfere with lipid metabolism.
Clinical and laboratory data were retrieved from patients’ folders and from a computerized data base obtained from the National Health Laboratory Services (NHLS). The data collected was: the study participant’s age, sex and baseline date (date when PIs treatment was started); serum TC, serum TG, CD4 count and viral load. Abnormal lipid profile was defined in accordance with NHLS guidelines, as: TC ≥ 200 mg/dl / 5.17 mmol/L, TG ≥ 150 mg/dl/1.69 mmol/L.
The statistical methods used to address the research questions included a repeated measures analysis of variance to compare later values with baseline values, log transformations (logs) to make the responses closer to normal distributions, and the nonparametric Friedman’s test for cases where the log transformation was not adequate for getting the data closer to normal. Since values at later times were supposed to be compared to baseline values, adjustment for multiple comparisons was done using Dunnett’s method. Adjusted p-values less than 0.05 were considered significant.
Ethical considerations
This study was approved by the ethics committee of the University of the Western Cape (Reference no. 12/5/7). Permission to conduct the study was granted by the Western Cape Department of Health (ID no. 10317) and the managers of the hospital /community health centres. It was conducted according to the ethics requirements of the South African Department of Health and the Declaration of Helsinki [10]. The information collected was kept confidential and saved in a safe file which could only be accessed by the researcher. Patient confidentiality and privacy were maintained at all times.
Results
A total of 753 patients including 491 (65.20 %) females and 262 (34.79 %) males were involved in the study. In the age group of 0-17 years there were 176 (23.37 %) patients, of whom 106 were females and 70 were males. In the age group 18-44 years, there were 465 (61.75 %) patients, of whom 322 patients were females and 143 were males. In the age group equal and above 45 years of age, there were 112 (14.87 %) patients including 63 females and 49 males.
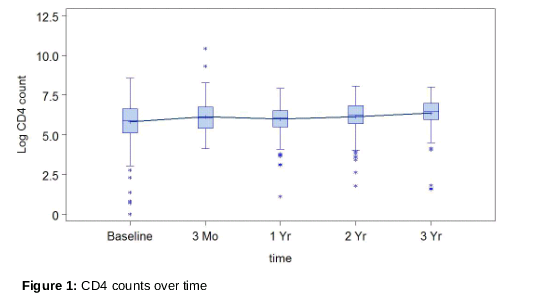
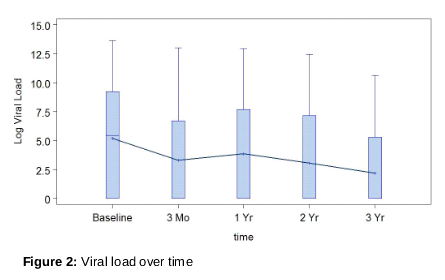
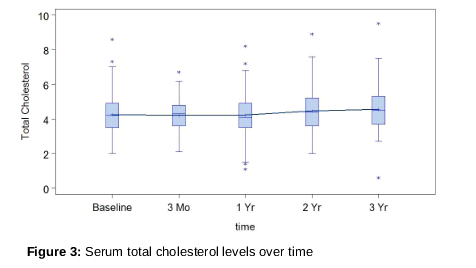
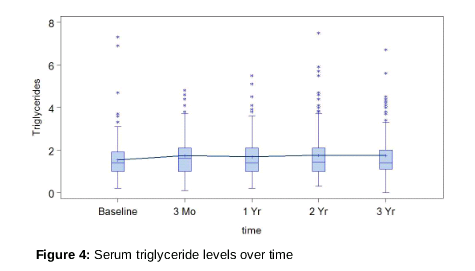
The CD4 counts, viral loads, serum TC and serum TG results are summarized in , 2, 3 and 4. Figures 1, 2, 3, and 4 show boxplots with a reference line joining the mean values for each time. The x-axis shows the times (baseline, 3 months. 1, 2 and 3 years after the start of PIs “treatment”. The y-axis shows the log values of the CD4 counts (), viral loads (), serum TC () and serum TG ().
Out of 753 patients, 59 (7.83 %) and 70 (9.29 %) had respectively serum TC and serum TG higher than normal values at baseline.
At baseline the level of compliance with therapeutic laboratory monitoring protocols recommended by the DOH were 23.24, 24.04, 47.41 and 36.79 % for serum TC, serum TG, CD4 counts and VL respectively. Three months after the beginning of the treatment, the levels of compliance with therapeutic laboratory monitoring decreased to 16.33, 17.66, 27.76 and 27.22 % for serum TC, serum TG, CD4 counts and VL respectively. One year after the start of PIs treatment, the level of compliance increased to 25.90, 24.83, 33.86 and 38.25 % for serum TC, serum TG, CD4 counts and VL respectively. However, two years after the beginning of treatment, the level of compliance dropped to 18.99, 19.26, 25.10 and 25.23 % for serum TC, serum TG, CD4 counts and VL, respectively.
For CD4 (), a log transformation was used, demonstrating that there were differences from baseline values. All comparisons with baseline values illustrated significant differences. However, examination of the residuals indicated a lack of normality. Consequently Friedman’s nonparametric test was done. Based on this test there were significant differences from baseline at all times: 3 months, 1, 2 and 3 years after the start of the treatment.
For viral load (), log transformation was used. All comparisons with baseline were significant. However, examination of the residuals indicated a lack of normality. Consequently, Friedman’s nonparametric test was done. Based on this test there were significant differences from baseline at all times: 3 months, 1, 2 and 3 years.
For serum TC (), there was a significant overall time effect (p=0.0061) with a significant difference from baseline at three years (adjusted p = 0.0137).
For serum TG (), a log transformation was used. The overall time effect was not significant (p=0.4132).
The mean values for serum TC at baseline were less than 4.5 mmol/L, and so were within the normal ranges. The values then slightly fall below 4 mmol/L at three months. From one year onwards during PIs treatment, the values increased minimally above 4 mmol/L but they were still within the normal ranges.
The mean values for serum TG at baseline () were also within the normal ranges -- less than 1.7 mmol/L. After three months of PIs treatment, the values surged above the normal values.
Tests were done to find out if sex and age might be related to the TC and TG values at any time. No significant relationships were seen.
Discussion
In this study, female and male patients were well represented in all age ranges. The high TC and TG serum levels observed in some patients at baseline were most likely due to either primary hyperlipidaemia or to previous exposure to drugs (eg. NRTIs in adult patients) that could alter the lipid profile. It could also be due to a decreased liver function [1]. Liver function tests results were not available to rule out that possibility.
Previous studies have reported menopause - induced reduction of HDL-cholesterol, and elevation of TC, TG, LDL -cholesterol and VLDL-cholesterol [11]. In this study, there was no significant difference in TC and TG serum levels between males and females within this age range, suggesting that female hormonal changes did not influence lipid levels.
This study demonstrated a significant difference in TC serum levels between baseline and 3 years. TG serum levels did not significantly change. According to Carr et al, PIs may not be the only class of antiretroviral medication associated with dyslipidaemia [2]. NNRTI therapy was associated with hypercholesterolemia and a statistically significant linear, temporal increase in serum TC levels. However, the effect of NNRTIs on TC serum levels was weaker than the effect of PIs [2].
The trend indicates that the longer the patient is exposed to PIs, the more CD4 cell counts increase, and viral load decreases. TC serum levels increased, as a consequence of the aforementioned trend. Although treatment with PIs contribute to patient susceptibility to metabolic disorders such as dyslipidaemia, they have also improved the prognosis of HIV infection in the HIV clinics where the study was conducted.
The increase in serum TG levels reported in could be induced by PIs or due to dietary lifestyles of patients. After one year, the values slightly decreased and this may be as a result of initiation of lipid lowering therapy. After two years, the values moderately increased above normal values and remained constant up to three years of treatment. The results thus indicate that there was no hyperlipidaemia at baseline.
The observed lack of compliance with therapeutic laboratory monitoring guidelines can be attributed, on one side, to health professionals who did not collect blood samples for laboratory tests and, on the other, to patients who did not keep their appointments. Consequently, it will be difficult to detect cases of dyslipidaemia which may lead to severe cardiovascular complications if not treated.
Limitations of the study
The following unforeseen problems were encountered: poor laboratory results reporting and recording in the patient’s folder, poor administration of patient folders, and lack of knowledge of the extent to which 1st line ARV may have induced hyperlipidaemia.
Conclusion
This study demonstrates a significant increase in TC serum levels due to PIs, but increase in TG serum levels is not evident. Age and sex do not have any effect on both TC and TG serum levels. Compliance of patients and/or health care professionals with DOH protocols on laboratory monitoring of HIV infection therapy is poor.
Declarations
Acknowledgement
References
Archives


News Updates